

Introduction
Depression is characterized by physical and cognitive maladjustment, manifesting as feelings of sadness, emptiness, or irritability [1]. These emotional experiences can lead to feelings of frustration, guilt, worthlessness, and hopelessness [2]. If left unaddressed, persistent depression can escalate into clinical depressive disorders or even ideation of suicide [3]. Notably, depression is a significant risk factor for suicide, with suicidal ideation being one of its most potent catalysts [4]. Based on a 2022 press release by the Health Insurance Review & Assessment Service, the number of people with depression is projected to increase by 35.1% in 2021 compared to 2017 [5]. Consequently, the management of depression in individuals with depressive symptoms becomes imperative.
Exercise stimulates norepinephrine release, enhancing mood and effectively preventing and treating depression. A meta-analysis focusing on exercise and depression demonstrated its efficacy in treating clinical depression. It highlighted the potency of aerobics exercise in preventing and treating depression among older people [6, 7]. Among various aerobic exercises, walking is a safe and suitable physical activity for people of all ages. It is inherently natural, easy to execute, and allows for intensity adjustment while exerting minimal physical stress on joints, compared to other ground-based aerobic exercises, like running and climbing [8]. Walking is a safe and cost-effective aerobic option, without financial burden, and constitutes a foundational human physical activity [9]. In addition, daily walking exercises can improve mood, restore sleep, and alleviate physical conditions caused by stress unknowingly [10].
Particularly, walking has been shown to improve lower extremity strength, flexibility, postural stability, balance, and gait, which are important for fall prevention; improve cardiopulmonary function, prevent cardiovascular disease and diabetes, promote bone metabolism and smooth hormone secretion, reduce the risk and progression of dementia and ParkinsonŌĆÖs disease, strengthen the immune system, and reduce the risk of cancer owing to healthy lifestyle choices [11]. Furthermore, it is also recommended to improve the physical and psychological health of older people because it reduces depression, stress and improves their quality of life [12-17]. Therefore, walking should be encouraged among both young and older people.
A meta-analysis is a systematic method that uses quantitative data to synthesize and understand multiple studies on the same topic [18]. This approach statistically synthesizes the results of individual empirical studies and has the advantage of further organizing and generalizing the knowledge in a particular field [19]. Specifically, the sample size significantly affects the results of statistical hypothesis testing, accounting for most quantitative studies. As arbitrary interpretation of significant probability becomes a criticism among many researchers, meta-analysis is gaining attention as a new research method that can overcome the shortcomings of individual studies [20].
This meta-analysis aimed to provide objective and comprehensive evidence for the effectiveness of walking on depression. The results of this study provide a meaningful basis for confirming the significance of depression as an important component in planning and implementing effective walking programs.
Methods
Data Search
The literature search covered theses and dissertations published in Korea until June 2023. The academic databases used for the literature search were DBpia, Korean Studies Information Service System, National Assembly Library, and Research Information Sharing Service. We conducted a literature search on the effects of walking exercise on depression, querying ŌĆśwalkingŌĆÖ within each academic database and performing a search within the result for ŌĆśdepression.ŌĆÖ
Selection Criteria
The inclusion criteria for the analyzed articles were selected according to PICOS, and the literature was searched [21]. First, all the participants were people. Secondly, the treatment method and program (intervention) included walking exercises. Third, the control group did not perform walking exercises. Fourth, depression was the outcome measure. Fifth, the study was designed as a two-group post-test. Sixth, the dissertation was prioritized in case of duplication of theses and dissertations.
Selection Process
For the meta-analysis investigating the effects of walking exercise on depression, we searched various academic databases comprehensively. We found 99 dissertations and 91 journal articles in DBpia, 45 journal articles in the Korean Studies Information Service System, 14 dissertations and 28 journal articles in the National Assembly Library, and 187 dissertations and 110 journal articles in the Research Information Sharing Service. We excluded 112 duplicate dissertations and 150 journal articles, categorizing them based on title and abstract. This categorization led to the exclusion of 177 dissertations and 105 journal articles. Subsequently, we conducted a comprehensive review of the remaining literature, excluding four duplicate publications, five with inconsistencies in measurement variables, four displaying irregularities in analysis methods, and two unavailable fulltext articles. Finally, we selected 3 dissertations and 12 journal articles. The literature selection process is visually shown in <Figure 1> through a PRISMA flow diagram [22].
Coding
Author, year of publication, publication type, participant, sex, age of experimental and control groups, and depression instrument were coded as shown in <Table 1>.
The depression assessment instruments used in the reviewed literature were the BDI, CES-D, GDS, GDSSF-K, SCL-90-R-K, and SDS, with adaptations and occasional utilization of abbreviated versions. The Beck Depression Inventory (BDI) consists of 21 questions regarding emotional, physiological, cognitive, and motivational symptoms, with higher scores indicating more severe depression. It can be administered in a short time, is inexpensive, easy to administer, can be scored, can be used in groups, and has high reliability, validity, and sensitivity. Scores ranged from 0ŌĆō63, with 0ŌĆō9 categorized as not depressed, 10ŌĆō15 as mildly depressed, 16ŌĆō23 as moderately depressed, and 24 or more as severely depressed.
The CES consists of 20 questions with a maximum score of 60, with higher scores indicating more severe depression. A score of 15 or less indicated no depression, 16ŌĆō20 indicated mildly depressed, 21ŌĆō24 indicated moderate depression, and 25 showed severe depression. The Geriatric Depression Scale (GDS) is a 30-item questionnaire with ŌĆ£yes/noŌĆØ responses. Higher scores indicate more severe depression, with 0ŌĆō9 indicating no depression, 10ŌĆō19 indicating mild depression, and 20 or more indicating severe depression. The shortened version of the GDS consists of 15 questions, with scores less than 5 indicating no depression, 5ŌĆō9 indicating mild depression, and 10 or more indicating severe depression.
The SCL-90-R-K is a short-form psychiatric diagnostic test consisting of 13 questions on depression that are scored on a 5-point scale. The measured score, which varied from 34ŌĆō92 and represented a conversion of the T-score from the normative table for the general population, indicated higher levels of depression. The Self-Rating Depression Scale (SDS) is a 20-item, 4-point scale. The maximum score was 80, with a score of 49 or less categorized as not depressed, 50ŌĆō59 as mildly depressed, 60ŌĆō69 as moderately depressed, and 70 or more as severely depressed.
Specific criteria for coding must be provided, and inter-rater agreement and reliability must be verified before conducting a meta-analysis [23]. To this end, data coding of the selected articles was conducted by one sports psychology doctor and a sports psychology professor with experience in meta-analysis research. A sports psychology doctor was consulted in case of data coding discrepancies.
Statistical Analysis
Meta-analysis was performed using the R meta-analysis package (ver.4.3.1). Effect sizes were calculated as standardized mean differences (SMD) using the post-hoc means and standard deviations of the experimental group with walking exercise, the control group without walking exercise, and the number of participants. The standardized mean difference allows different measures to be standardized to a single unit and evaluated using the same outcome variables. The operational definition of the standardized mean difference used in Cochrane Reviews is the effect size known in the social sciences as HedgesŌĆÖ g [24]. CohenŌĆÖs d is a measure of the sample size. Because CohenŌĆÖs d tends to overestimate the effect sizes when the sample is small, it must be converted to HedgesŌĆÖ g, which is correct for studies with large and small samples [25]. The confidence interval (CI) for the effect size is 95%, and an effect size of 0.2ŌĆō0.5 was interpreted as a small effect size, 0.5ŌĆō0.8 as a moderate effect size, and greater than 0.8 as a large effect size [26].
The I2 value was used to test the heterogeneity of studies. An I2 of 25ŌĆō50% was considered low heterogeneity, 50ŌĆō75% was considered moderate heterogeneity, and 75% was considered high heterogeneity [23]. In general, heterogeneity was judged to be significant if the ratio of true variance to total variance (I2) was greater than or equal to 50% and the significance probability of the homogeneity test was less than .10 [23]. We chose a random-effects model if the analysis showed high heterogeneity among the studies and a fixed-effects model if the analysis showed low heterogeneity.
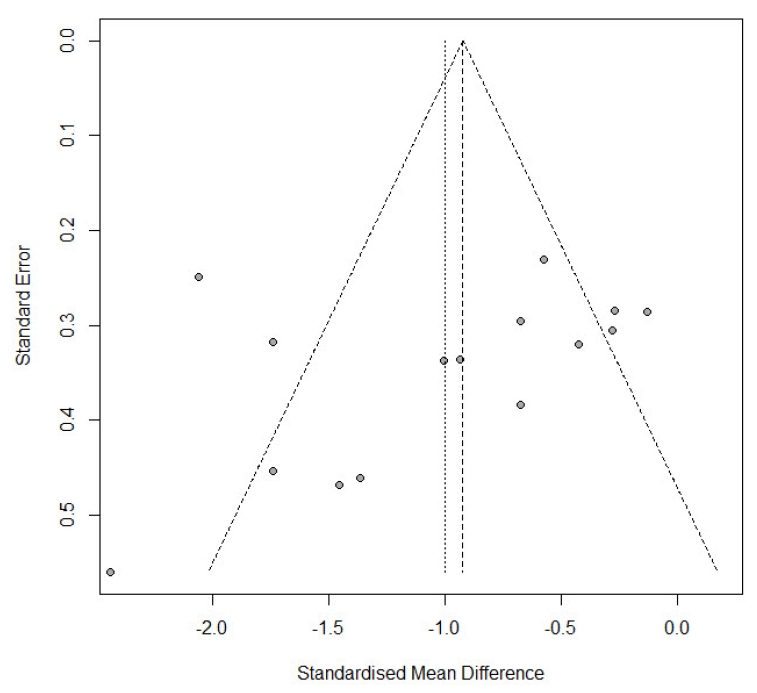
To verify the validity of each study, we constructed a funnel plot and Egger regression analysis to verify publication bias [27].
Results
Publication Bias
Funnel plots and Egger regression tests assessed publication bias. The funnel plot visually examines, while EggerŌĆÖs regression test offers a statistical evaluation. The funnel plot of selected literature for the meta-analysis of walking exercise effects on depression is shown in <Figure 2>. Regression analysis showed a bias of-3.0048 (t=-1.26, df=13, p=0.2307), indicating no publication bias.
Effect Size
The meta-analysis result on the effect of walking exercise on depression is shown in <Figure 3>. A random-effects model was employed due to the high heterogeneity among the studies (I2=78%, p<.01). The effect size was -1.00 (95% CI=-1.35, -0.65), indicating a large effect size with a significant difference (z=-5.56, p=.0001). Walking was also found to affect depression.
Discussion
This study conducted an extensive meta-analysis of theses and dissertations to comprehensively analyze and identify the effects of walking as an exercise on depression. Based on the defined selection criteria, 15 articles were chosen, including three dissertations and 12 academic articles. The meta-analysis yielded an effect size of -1.00, indicating a significant effect. A negative mean difference indicates a decrease in depression level, with higher scores reflecting increased severity. Therefore, walking was found to affect depression.
National and international studies have shown the effective reduction of the negative emotions of depression through walking [28, 29]. Moreover, studies that have examined the relationship between physical activity and depression have reported that both the duration and intensity of physical activity can reduce depression [30]. Our findings also suggest that walking exercise has a positive effect on depression. However, the results may vary depending on the intensity and duration of the walking program and the participantsŌĆÖ health characteristics and size [31-33].
Upon examining the age of unaffected participants in the studies selected for the meta-analysis, we identified a positive effect of walking on depression among older participants [34-43] and middle-aged housewives [44]. However, a study involving middle-aged office workers reported only a small effect of walking on depression [41]. When comparing intervention durations, the study of middle-aged housewives was conducted three times a week for 15 weeks, totaling 45 sessions [44]. In contrast, the study of middle-aged office workers was conducted twice a week for five weeks, totaling 10 sessions [41], which may explain the shorter duration and frequency of the intervention. Moreover, a study of middle-aged housewives [44] clearly set the intensity of the walking exercise, but a study with middle-aged female workers of [41] did not set the intensity of the walking exercise. Hence, it is necessary to apply not only the duration and frequency of walking, but also the intensity according to the characteristics of the participants.
Among the studies selected for the meta-analysis, walking exercise positively affected depression in one study on patients with cancer [45] and patients with diabetes [28]. In a study with stroke patients [46], depression levels at the pre-intervention were normal in both the exercise and control groups. However, after the intervention, the exercise group showed no change in depression scores, while the control groupŌĆÖs depression scores increased to mild-to-moderate levels. This pattern indicates that walking is a positive intervention program. It can be inferred that these results are due to the participantsŌĆÖ health characteristics and that the walking programŌĆÖs intensity and duration should be adjusted accordingly.
Depression is a marker of mental health and is strongly associated with physical and mental performance, subjective health, and happiness [47, 48]. Moreover, depression is strongly associated with suicide, necessitating efforts to reduce its impact. Meta-analyses have shown that walking, as a means of reducing depression, has a positive effect. Considering the characteristics of participants and their level of depression, it is necessary to consider the interventionŌĆÖs duration, frequency, and intensity, especially given that not all studies have shown a positive effect on depression.
Conclusions
This study conducted a meta-analysis to objectively determine the effects of walking on depression. The results showed that walking exercise has a positive impact on depression. This study validates the effectiveness of walking exercises and provides a basis for developing programs to reduce depression.
While this study presents significant conclusions, it has some limitations. First, the study only compared the effects of walking exercise on depression; therefore, the interventionsŌĆÖ duration, frequency, and intensity were not considered. Second, the studies included in this meta-analysis predominantly involved older women. Therefore, it is necessary to include studies involving different age groups. Future studies should address these limitations to provide more systematic and comprehensive conclusions regarding the effects of walking on depression.