
Introduction
Anterior knee pain (AKP) is a common musculoskeletal problem in individuals that one-fourth of people experience at least once in their lives [1]. Patients complain of peripatellar or retropatellar pain during daily (e.g., squatting, kneeling, and stair walking) [2] and athletic (e.g., running, jumping, landing) movements [3]. To control pain, therapeutic modalities such as high-frequency transcutaneous electrical nerve stimulation (TENS) and focal joint cooling are commonly used. Due to anaesthetic effect, the use of these modalities allows voluntary contraction and active movements— called cryokinetics [4].
Conservative therapeutic exercises for AKP include the restoration of quadriceps function [2] and strength development of the lower extremity [5] . Quadriceps inhibition is thought to be the result of reduced motor signals due to abnormal afferent sensory input stemming from the painful area (e.g., knee joint) [6]. Since the 2000s, a disinhibitory effect (e.g., reversal of neural inhibition in quadriceps) on TENS and focal knee joint cooling has been reported in controlled laboratory studies using an experimental injury model [7], as well as in clinical studies with knee pathologies [8, 9]. Theoretically, disinhibition provides a clinical situation where patients would be able to recruit more active motor units [10]. Therefore, reversing neural inhibition (by using modalities) prior to performing voluntary exercises is suggested as a course of action [11].
Strength development in the quadriceps and lower-extremity is typically guided for pain reduction and functional improvement in rehabilitation of AKP [11]. To accomplish this, a fixed external weight should be incorporated throughout the available range of motion (ROM) [10]. When performing resistance exercises for the isolated contraction of the quadriceps [12] or co-contraction with other muscles [13], the use of the daily adjustable progressive repetitive exercise (DAPRE) technique [14] is recommended. To maintain or improve the cardiorespiratory system to transfer the necessary oxygen supply to the working tissues, whole-body exercise is performed. This type of exercise is referred to as “aerobic exercise” and is typically performed as a warm-up activity. Considering the restrictions in the hip joint ROM [15, 16], flexibility exercises focusing on the hip flexors and extensors are also recommended.
While well-designed programmes and appropriate progressions in the interventions described above are keys to a successful rehabilitation outcome, no information regarding the degree of change or progression during multiple sessions of rehabilitation. Pain reduction and strength development are expected, it is unclear when and how such progressions occur. Clinicians and patients would benefit from referencing and applying such information when establishing and implementing each rehabilitation component. Therefore, the purpose of this study was to report changes in pain perception and the TENS pulse amplitude, and progressions in aerobic and resistance exercise at each session during a ten-session rehabilitation programme for patients with AKP. As secondary outcomes, hip joint flexibility (hamstring and iliopsoas muscle lengths) on each side and functional outcomes (Kujala AKP scale) [17] were assessed.
Methods
Participants
Fourteen patients with AKP were initially recruited, educated about the study, and then gave informed consent (approved by the University’s Institutional Review Board: approval No. KHSIRB-18-002); however, three dropped out due to scheduling conflicts (n=2) and low back pain (n=1). The data of eleven patients <Table 1>, therefore, were finally analysed in this observational study.
Eligible AKP patients were those who reported feeling pain for at least two months during at least two of the following activities: (i) ascending or descending stairs, (ii) sitting for longer than an hour, (iii) contraction of the quadriceps, or (iv) patella compression while sitting with the leg extended [2]. Additionally, patients had to report their pain perception as greater than 2 out of 10 cm on a visual analogue scale (VAS) during daily activities to be included [16].
Patients with a history of musculoskeletal surgeries or a diagnosis (physician confirmed) of osteoarthritis or rheumatoid arthritis, epilepsy or seizures, patellofemoral dislocation or subluxation, any neurological disorder, diabetes mellitus, or pregnancy were excluded.
Rehabilitation Programme
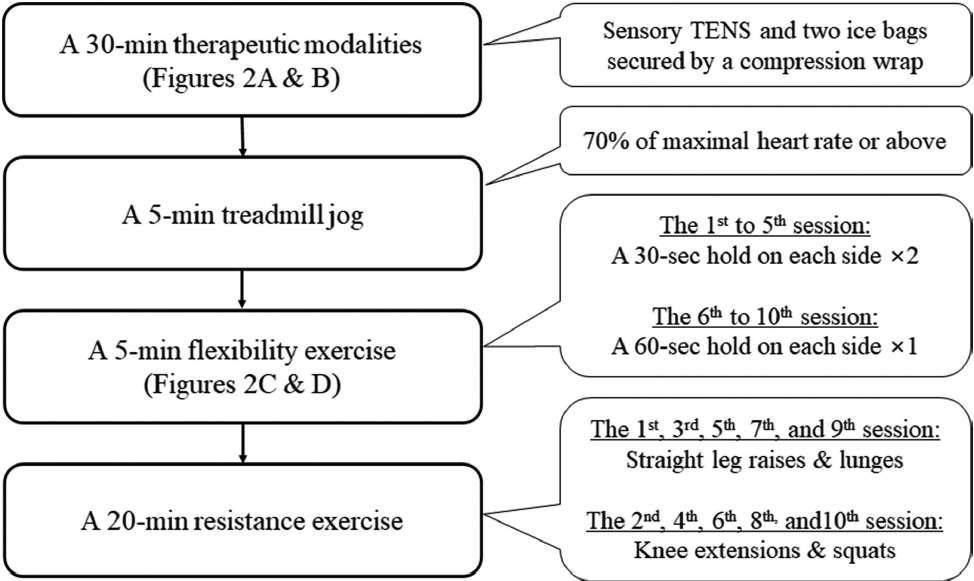
Patients participated in ten sessions of the supervised rehabilitation programme <Figure 1>, separated by two days (maximum of 72 hours). Each rehabilitation session was completed in the order of a 30-min electro-cryotherapy followed by another 30-min of exercises. All rehabilitation exercises were administered by research assistants. Prior to the first rehabilitation session, research assistants were educated on the correct techniques and safety considerations for each exercise.
Electro-cryotherapy
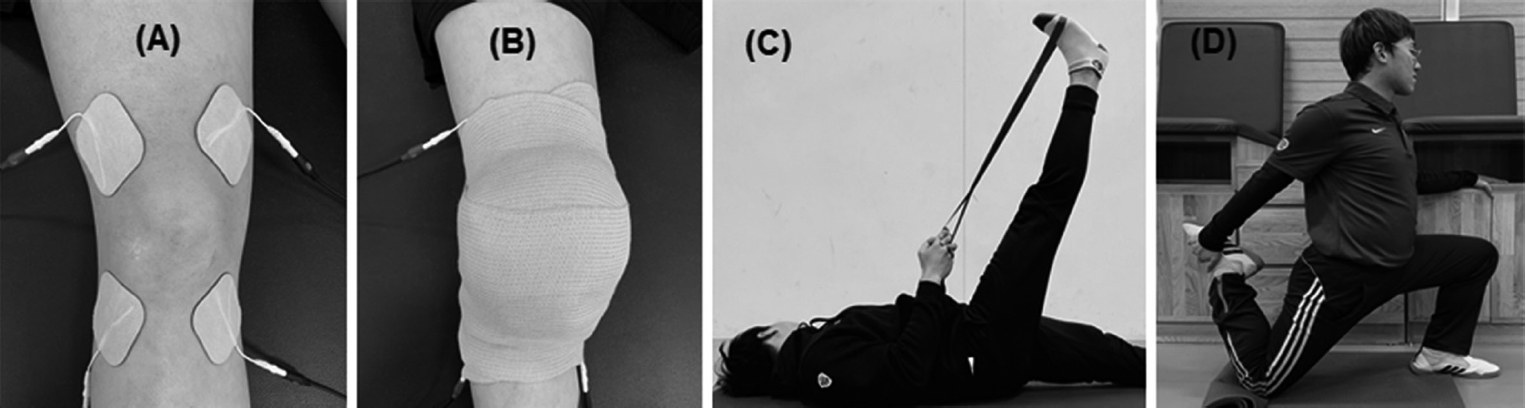
Upon arrival at the clinic for each session, patients were asked to mark where their perception of their pain (e.g., daily activity) was on a 10-cm VAS. Afterwards, a 30-min electro-cryotherapy was applied. A longer duration (45-min) of TENS has shown to produce a better outcome [8], the 30-min duration was determined due to our one-hour rehabilitation. Two channels (four electrodes: 5 × 5 cm self-adhesive squared) of TENS current (TENS 3000: 0-80 mA peak amplitude and 500 ohm, Koalaty Products Inc., Tampa, USA), were crossed to target the painful knee joint <Figure 2A>. Specifically, the electrodes of one channel were attached on the distal vastus lateralis and the medial aspect of the proximal tibia and those for another channel were attached on the vastus medialis and the lateral aspect of the proximal tibia. Two ice bags (size: 25 × 45 cm; filled with 500 mL of crushed ice) were then applied to the anterior and posterior aspects of the painful knee joint, secured by an elastic wrap bandage <Figure 2B>. The stimulus intensity (pulse amplitude) of TENS (asymmetric biphasic current; frequency: 150 Hz; pulse duration: 150 μs) was then gradually increased up to a point where patients tolerated the electrical discomfort without a visible quadriceps contraction. The determined TENS pulse amplitude was maintained at the session and recorded.
Aerobic Exercises
Patients performed treadmill jogging (Jog Forma, Technogym S.p.A, Gambettola, Italy). Patients jogged at a speed of 6.0 (females) or 7.0 km/h (males) for the first session (0% inclination was used throughout the rehabilitation programme). The treadmill speed was determined by a pilot work (2 females and 2 males). After 3-min of jogging, patients were asked to firmly grip the heart rate sensor handlebars (mounted on the treadmill) until the highest heart rate value did not change for 10-sec. Our pilot study (2 females and 2 males) showed a high correlation (r=0.77, p<0.0001) with this measurement and a simultaneously recorded heart rate measurement gathered via a chest strap (Polar H10, Polar Electro Inc., NY, USA). A value of 70% of the age-based maximal heart rate estimation ([220 – age] × 0.7) [18] was used as a threshold for the progression of treadmill speed. When patients did not reach 70% of their maximal heart rate at 3-min after jogging (assuming that the given treadmill speed did not require a certain energy level), a speed increase of 0.5 km/h was added at the next session. The treadmill speed at each session was recorded.
Flexibility Exercises
For hip joint ROM, the hamstring (flexion <Figure 2C>) and iliopsoas (extension <Figure 2D>) were self-stretched. The stretching intensity (where the stretching force to elongate muscle tissue stops) was subjectively determined by the point at which patients equally felt stretching and discomfort. Patients (n=2) with knee pain due to pressure on their knees in the position of iliopsoas stretching were instructed to stretch while adopting the modified Thomas test position [15]. Stretching exercises were initially performed twice with a 30-sec hold on each side for the first five sessions, which then progressed into a 60-sec hold with the same intensity and sets for the last five sessions <Figure 1>. Before and after the ten-session rehabilitation programme, the hip joint ROM was measured (by a same researcher) using a plastic goniometer with the positions of straight leg raise (SLR) for hip flexion ROM [19] and modified Thomas test for hip extension ROM [15].
Resistance Exercises
Patients performed a pair of SLRs and lunges, and single-knee extensions and squats were completed. Due to the time limitation (20-min) of this exercise component, resistance exercises were performed alternatively during each session. For example, SLRs and lunges were performed at the odd-numbered session while knee extensions and squats were performed at the even-numbered session <Figure 1>. Except for the SLRs, a stack machine (single knee extensions) and a Smith-type machine (lunges and squats) were used (Technogym S.p.A, Gambettola, Italy). If the repetitions exceeded eight, a 5 kg weight plate was added [14]. To report progression in resistance exercises, the working weight as an external load that patients resisted for single-knee extensions, lunges, and squats were recorded in kg during each session.
After each session, the pain perception was obtained again in the same manner described above. Before and after the rehabilitation, patients completed the Kujala AKP scale.
Statistical Analysis
Sample size estimation was calculated using the given outcome variable of quadriceps function as in a previous report [20], where a change in quadriceps central activation ratio of 0.06 with a standard deviation of 0.1 (effect size of 0.6) has been reported. Based on this expected difference, with an alpha of 0.05 and a beta of 0.2, the results were calculated that a minimum of 11 participants would be necessary.
As the primary outcomes, pain perception was recorded before and after each session (treatment × session: 2 × 10). The TENS pulse amplitude and jogging speed were also recorded at each session (session effect: 1 × 10). Finally, the external loads that patients had to exert for lunges and single knee extensions on each side (session × leg: 5 × 2), and for squats (session effect: 5 × 1) were also recorded at each session. As the secondary outcomes, hip joint ROM (hamstring and iliopsoas flexibility) on each side (rehabilitation × leg: 2 × 2) and the functional outcome measures (rehabilitation effect: 1 × 2) were assessed before and after the ten-session rehabilitation programme.
Two-way analysis of variance (pain perception, resistance exercise, and hip joint ROM), one-way analysis of variance (TENS pulse amplitude and jogging speed), and a t-test (functional outcome measures) were performed along with Tukey-Kramer pairwise comparisons for post-hoc tests (p<0.05 for all tests; SAS 9.4, SAS Institute Inc., Cary, NC, USA). When statistical significance was detected, Cohen’s d effect sizes (d = [ 1 – 2] / σpooled) was calculated.
Results
Primary Outcomes
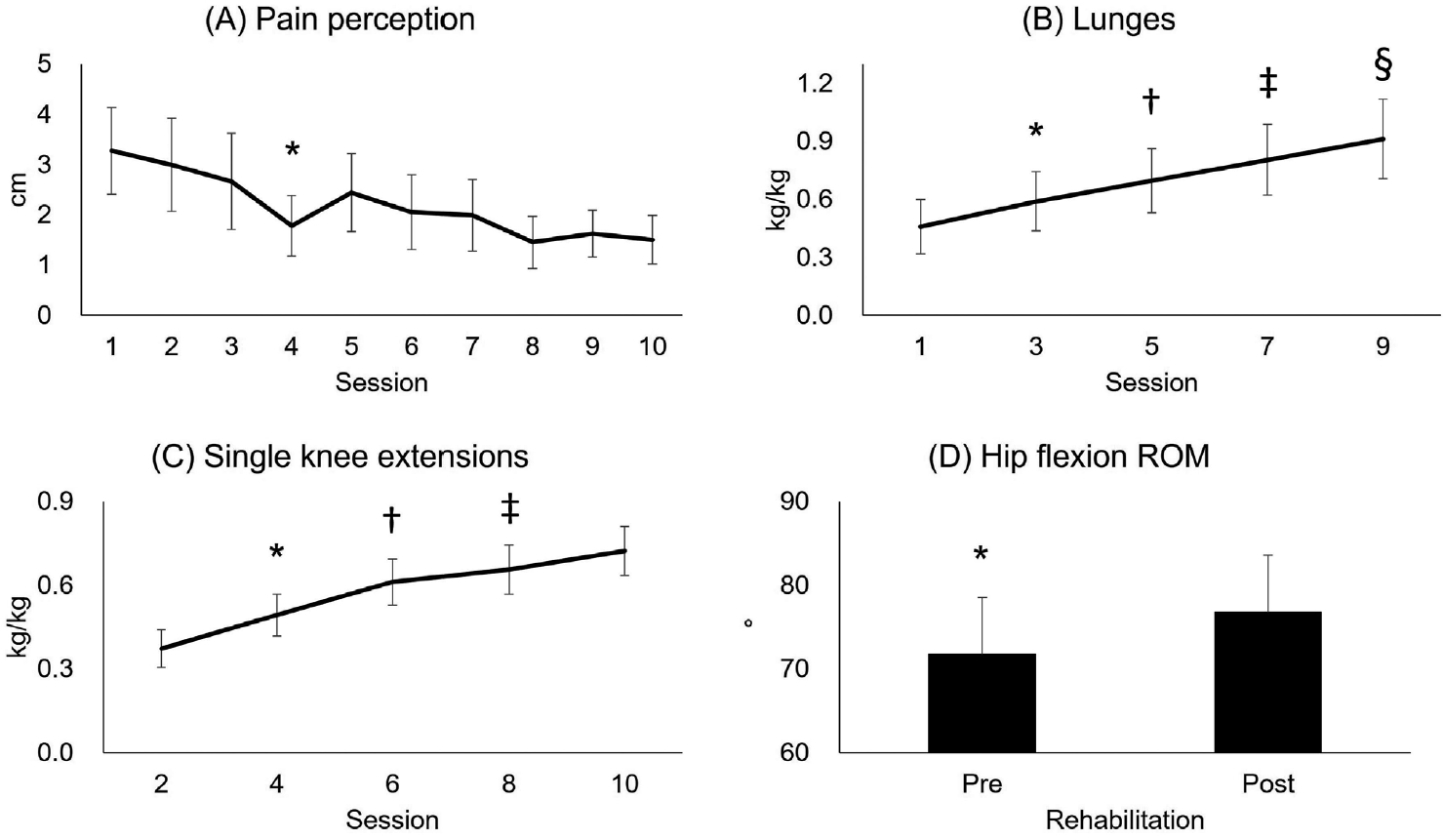
There was no treatment effect over ten-sessions for pain perception (treatment × session: F9,190=0.32, p=0.97) <Table 2>. Pain perception between pre- and post-treatment did not differ (treatment effect: F1,190=1.24, p=0.27), indicating that a single session of treatment did not reduce the pain perception. However, regardless of treatment (session effect: F9,190=4.31, p<0.0001), pain perception was decreased at the 4th session (p=0.03, d=0.84) <Figure 3A>.
The TENS pulse amplitude was increased at the 7th session (p=0.03, d=1.04), but there was no further change observed thereafter (session effect: F9,90=2.27, p=0.03) <Table 2>.
Treadmill jogging speed (session effect: F9,90=21.43, p<0.0001) was increased at the 4th (p=0.003, d=1.22) and further increased at the 8th (p=0.006, d=0.72) session <Table 2>.
There was no session effect on the leg during lunges (session × leg: F4,90=0.91, p=0.46; leg effect: F1,90=3.72, p=0.06) <Table 3>. Regardless of leg (session effect: F4,90=284.49, p<0.0001), the external load of lunges improved every session <Figure 3B>. Specifically, it increased at the 3rd (32.7 to 41.8 kg, p<0.0001, d=0.53), the 5th (49.4 kg, p<0.0001, d=0.39), the 7th (57.1 kg, p<0.0001, d=0.37), and the 9th session (64.4 kg, p<0.0001, d=0.32). There was no session effect on the leg during single-knee extensions (session × leg: F4,90=0.13, p=0.97; leg effect: F1,90=3.86, p=0.06) <Table 3>. Regardless of leg (session effect: F4,90=115.84, p<0.0001), external loads during the single-knee extension exercises improved at the 4th (26.4 to 34.7 kg, p<0.0001, d=1.00), the 6th (43.2 kg, p<0.0001, d=0.89), and the 10th (51.0 kg, p=0.004, d=0.77) session <Figure 3C>. The external loads of squats were increased every session (session effect: F4,40=161.95, p<0.0001) <Table 3>. Specifically, it increased at the 4th (34.5 to 46.0 kg, p<0.0001, d=0.84), the 6th (56.4 kg, p<0.0001, d=0.74), the 8th (66.1 kg, p<0.0001, d=0.66), and the 10th session (73.8 kg, p=0.0006, d=0.51).
Secondary Outcomes
There was no leg effect over rehabilitation in hip flexion ROM (rehabilitation × leg: F1,30=0.07, p=0.80; leg effect: F1,30=0.01, p=0.96) and hip extension ROM (leg × rehabilitation: F1,30=0.43, p=0.52; leg effect: F1,30=3.04, p=0.09; rehabilitation effect: F1,30=3.30, p=0.08) <Table 4>. Regardless of leg, hip flexion ROM (hamstring flexibility) increased by 5.1° (rehabilitation effect: F1,30=8.65, p=0.006, d=0.44) after the rehabilitation <Figure 3D>.
After ten-sessions of rehabilitation, the score of self-reported functional outcomes (Kujala AKP scale) improved by 17% (t=3.60, p=0.003, d=1.53) <Table 4>.
Discussion
We sought to report changes and progressions of changes in pain perception and the TENS pulse amplitude, and progressions in aerobic, flexibility, resistance exercise, and functional outcome measure during and after a ten-session rehabilitation programme for patients with AKP. Our data on pain perception showed that a single treatment was not effective to reduce the pain perception <Table 2>, but overall pain (collapsed on pre- and post-treatment in each session) was reduced by 49% at the 4th session <Figure 3A>. This indicates that multiple sessions are necessary to achieve a significant reduction of chronic AKP (pain duration: > 46 months), which is consistent with what previous studies have suggested [21, 22]. It should be noted that observed pain reduction in our study is the result of a combined effect on the rehabilitation programme. For example, the capacity of aerobic and resistance exercise increased at the 4th session <Tables 2 & 3>, which could certainly have contributed to pain reduction. While a pain perception greater than 3 cm on a 10 cm in VAS has been used as an inclusion criterion for clinical study of AKP [1, 23], the observed pain level at the 4th session from the baseline (3.4 to 1.7 cm, d=0.89) is clinically meaningful. Considering the data of increased capacities to perform aerobic and resistance exercises during the 2nd and 3rd sessions <Table 2 and Figure 3>, joint stability and movement efficiency in the lower extremity during daily activities could also be improved, which made patients relatively less conscious of their AKP. While the improved exercising capacities along with the pain reduction could have possibly led to a functional improvement, the relative effectiveness of the interventions (e.g., therapeutic modalities vs. rehabilitation exercises) is unclear. We think that the use of therapeutic modalities not only reduced pain perception but also facilitated voluntary exercises at each rehabilitation session, which could have improved lower extremity function.
There is a fading of electrical (tingling) sensation during and after receiving multiple treatments of TENS [24]. This response is attributed to accommodation (an increased threshold in depolorisation), adaptation (reduced subjective sensation), and habituation (reduced reaction of the central nervous system to action potential) [25]. There have been a couple of studies [26, 27] concerning the necessity of adjustment in TENS during a single-session intervention. In an earlier study [26], an adjusted amplitude resulted in an increased pain threshold as compared with fixed TENS. A recent study [27] did not report the superiority of adjusting a pulse amplitude over the fixed amplitude in terms of pain reduction. While the hypoalgesic effect of adjusting the amplitude is still under debate, we opted to increase it as tolerated every session because the adjusting amplitude method is usually practiced; there is insufficient evidence on the use of fixed amplitude. We observed a 20% increase in the pulse amplitude of TENS at the 4th session but no further increase thereafter. Previous studies similar to ours specified the adjustable range—up to 60 [28] or 80 mA [29]—for home training sessions but the amount of amplitude change was not reported. Therefore, our study is the first attempt to report the amount of adjustment in pulse amplitude of TENS application over multiple sessions in managing clinical knee pain. It should be noted that our observation was the change in pulse amplitude with a simultaneous application of knee joint cooling. This may explain why the highest amplitude was recorded as 31 mA in our data, while the adjustable range (60 and 80 mA) in previous studies [21, 28] were relatively larger.
Based on our progression criterion (simply calculated as > 70% of the age-based estimation on maximal heart rate), our participants showed an improvement on treadmill jogging speed at the 3rd, 5th, and 9th sessions (a total of 28% improvement) <Table 2>. Despite its popularity in rehabilitation, progression guidelines of aerobic exercise have not been suggested. Therefore, we were interested to report how patients with AKP responded to the exercise intensity determined by a simple progression criterion without using additional devices. As no data are available on the progression of aerobic exercise over multiple rehabilitation sessions, our data would be a possible future reference for clinicians and patients in this regard.
A progression in working weight during resistance exercises was observed at every session, indicating that a single session of our interventions could result in significant strength development AKP <Table 3, Figures 3B and C>. Our rehabilitation programme was designed to accomplish the previously suggested “open, then exploit” strategy [11]. The time (approximately 10-min) between the modality use and resistance exercises was a sufficient duration for the disinhibitory effect [8]. Since neural activation was not directly measured, it is unclear as to whether quadriceps disinhibition actually happened at the time of resistance exercises. However, the observed increase in working weight at every session, especially the first five sessions (less than two-weeks of duration) may be evidence of the process of reversing neural inhibition. This assumption is reinforced by the content of previous research: knee extension exercises alone did not show an immediate increase in quadriceps strength and activation [30]. Given the occurrence of the aforementioned disinhibitory strategy, we believe that the facilitation of movements during exercises by numbing the painful area using knee joint cooling [4] contributed to some extent.
There was an overall (regardless of side) 5.1° increase in hip flexion test results <Figure 2D>. The normative value in this test position in a similar age group was known as 74° [31] that our patients’ hamstring lengths were within normal range. While we believe that stretching exercises directly influenced hip flexibility, the observed outcomes should be interpreted as result of combined effects with other therapeutic exercises. A previously reported critical criterion for iliopsoas tightness was –9.7° [29], indicating that our patients’ iliopsoas were much tighter and the flexibility exercises did not change this. Unlike hamstring flexibility, the testing (modified Thomas test) and training positions <Figure 2D> for iliopsoas were different than exercising while applying the modified Thomas test and could have yielded a different result. Additionally, a greater stretching load may have been applied to the knee extensors than the iliopsoas by the half-kneeling exercise. We gave correct instructions and continuous feedback on this stretching position, but one-onone supervision was limited due to helping other patients with modality applications. Although the exact causality has not been determined, it is believed that the level of function and the severity of AKP is associated with hip joint flexibility [15, 19]. Therefore, stretching exercises targeting hip joint flexibility should be included in the exercise prescription for AKP patients. The Kujala AKP scale is a valid and reliable tool by which to assess the functional level for young adults with AKP. Previously, 20-sessions of exercise [32] and 60-sessions of exercise in conjunction with neuromuscular electrical stimulation [22] improved the Kujala AKP scale by 17% (60 to 73/100) and 18% (73 to 89/100), respectively. We also observed a 17% of improvement (73 to 89 /100) after ten-sessions of rehabilitation in our patients may suggest that our rehabilitation programme (in terms of components and the order) could be an optimal means for pain reduction and functional improvements.
Assumptions should be noted that (1) physiological and biomechanical adaptations of the rehabilitation programme were not different across patients and (2) the psychological factors such as cognitive appraisal, emotional changes, motivation, and adherence were also similar. Lastly, the design of this study is limited to determine the superiority or interrelationship of therapeutic interventions (e.g., therapeutic modalities, and aerobic, anaerobic, and flexibility exercise) in reducing pain perception and improving functional outcomes. We acknowledge that the observed changes and progressions in each rehabilitation component were somewhat affected by each other. For example, increased flexibility could have been involved with pain reduction, or vice versa. Future research should attempt to examine an isolated effect of each rehabilitative intervention.
Conclusions
The current study reported changes in pain perception and the TENS pulse amplitude, and progressions in aerobic and resistance exercise over a series of ten-session rehabilitation programme for patients with AKP. The observed changes and progressions could be used as general guidelines for the establishment and implementation of a short-term consecutive rehabilitation.